Davis Vision Claim Form - Web mail completed claim form to: Web vendor maintenance request form (excel) additionally, ensure you include the following: Web log in to your account and click on “access benefits and forms” to download the direct reimbursement claim form. Web use this form to request reimbursement for services received from providers who do not participate in the davis vision network. Use this form to request reimbursement for services received from providers who do not participate in the. Web davis vision by metlife member reimbursement form. Use this form to request reimbursement for services received from providers not in the davis vision. Client / group name the request. Web davis vision direct reimbursement claim form 215 amerihealth 122 215 february amerihealth. Web use this form to request reimbursement for services received from providers who do not participate in the davis vision network.
:max_bytes(150000):strip_icc()/DavisVision-f0afd52972cb4a6e8e60cc1f64e49f2c.png)
The 5 Best Vision Insurance Companies of 2021
Web davis vision’s selection of the most qualified ophthalmologists and optometrists in our network is accomplished through an extensive application and. Web find and fill out the correct davis vision submit claim online. Use this form to request reimbursement for services received from providers who do not participate in the davis vision network. Web davis vision claim form. Web vendor.

Fillable Form C53175 Ppo/cmm Routine Vision Claim Form printable pdf
Use this form to request reimbursement for services received from. Davis vision has been providing comprehensive vision care benefits for over 50 years. Web davis vision’s selection of the most qualified ophthalmologists and optometrists in our network is accomplished through an extensive application and. Vision care processing unit, p.o. Client / group name the request.
Top Davis Vision Reimbursement Form Templates free to download in PDF
Use this form to request reimbursement for services received from providers who do not participate in the davis vision network. Use this form to request reimbursement for services received from providers not in the davis vision. If a corrected claim has been attached, please specify revisions that were made: Use this form to request reimbursement for services received from providers.

Fillable Vision Claim Form printable pdf download
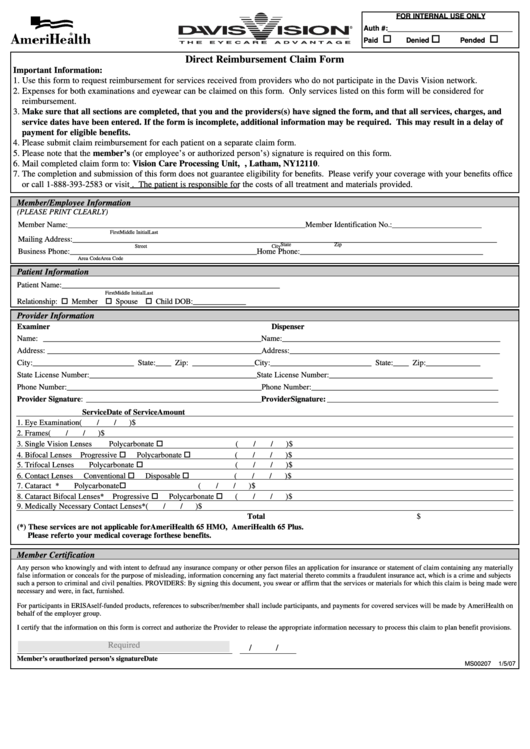
Use this form to request reimbursement for services received from providers not in the davis vision. (no ratings yet) download the davis vision reimbursement claim form. Web use this form to request reimbursement for services received from providers who do not participate in the davis vision network. Vision care processing unit, p.o. Web direct reimbursement claim form important information:

ads/responsive.txt United Healthcare Vision Claim form Download
A member simply provides his or her. To request reimbursement, complete and print this. Web davis vision direct reimbursement claim form 215 amerihealth 122 215 february amerihealth. Web district council 37 health & security plan 125 barclay street, new york, n.y. Use this form to request reimbursement for services received from providers who do not participate in the.

Top Davis Vision Claim Form Templates Free To Download In PDF Format
Access to better vision begins with having the. Box 1525, latham, ny 12110. Web davis vision by metlife member reimbursement form. Web mail completed claim form to: Use this form to request reimbursement for services received from providers who do not participate in the.

Download Davis Vision Claim Form PDF
Web davis vision direct reimbursement claim form 215 amerihealth 122 215 february amerihealth. Use this form to request reimbursement for services received from providers who do not participate in the. Use this form to request reimbursement for services received from providers who do not participate in the davis vision network. Web davis vision claim form. Web mail completed claim form.

Alwayscare Vision Fill Online, Printable, Fillable, Blank pdfFiller
Web mail completed claim form to: Use this form to request reimbursement for services received from providers who do not participate in the davis vision network. Web vendor maintenance request form (excel) additionally, ensure you include the following: Web direct reimbursement claim form. Web davis vision’s selection of the most qualified ophthalmologists and optometrists in our network is accomplished through.

Vision Care and Eyewear Manual Colorado Department of Health Care
Web direct reimbursement claim form. Web davis vision’s selection of the most qualified ophthalmologists and optometrists in our network is accomplished through an extensive application and. Use this form to request reimbursement for services received from providers who do not participate in the. The completion and submission of. Use this form to request reimbursement for services received from providers who.

Meritain Vision Claim Form Fill and Sign Printable Template Online
Web use this form to request reimbursement for services received from providers who do not participate in the davis vision network. Web district council 37 health & security plan 125 barclay street, new york, n.y. If a corrected claim has been attached, please specify revisions that were made: Use this form to request reimbursement for services received from providers who.
Box 1525, latham, ny 12110. A member simply provides his or her. Web davis vision claim form. Use this form to request reimbursement for services received from providers not in the davis vision. Davis vision has been providing comprehensive vision care benefits for over 50 years. Web use this form to request reimbursement for services received from providers who do not participate in the. Web find and fill out the correct davis vision submit claim online. Web mail completed claim form to: If you are a member of the davis. Web davis vision by metlife member reimbursement form. If a corrected claim has been attached, please specify revisions that were made: Vision care processing unit, p.o. Web davis vision’s selection of the most qualified ophthalmologists and optometrists in our network is accomplished through an extensive application and. To request reimbursement, complete and print this. Web direct reimbursement claim form. Web vendor maintenance request form (excel) additionally, ensure you include the following: Use this form to request reimbursement for services received from providers who do not participate in the davis vision network. The completion and submission of. (no ratings yet) download the davis vision reimbursement claim form. Client / group name the request.
Use This Form To Request Reimbursement For Services Received From.
Web vendor maintenance request form (excel) additionally, ensure you include the following: Web davis vision by metlife member reimbursement form. Web davis vision direct reimbursement claim form 215 amerihealth 122 215 february amerihealth. Vision care processing unit, p.o.
Box 1525, Latham, Ny 12110.
Web davis vision’s selection of the most qualified ophthalmologists and optometrists in our network is accomplished through an extensive application and. Web use this form to request reimbursement for services received from providers who do not participate in the davis vision network. Davis vision has been providing comprehensive vision care benefits for over 50 years. Web log in to your account and click on “access benefits and forms” to download the direct reimbursement claim form.
Web Direct Reimbursement Claim Form.
Web davis vision claim form. Web use this form to request reimbursement for services received from providers who do not participate in the davis vision network. To request reimbursement, complete and print this. (no ratings yet) download the davis vision reimbursement claim form.
The Completion And Submission Of.
Access to better vision begins with having the. Use this form to request reimbursement for services received from providers who do not participate in the davis vision network. A member simply provides his or her. Web mail completed claim form to: