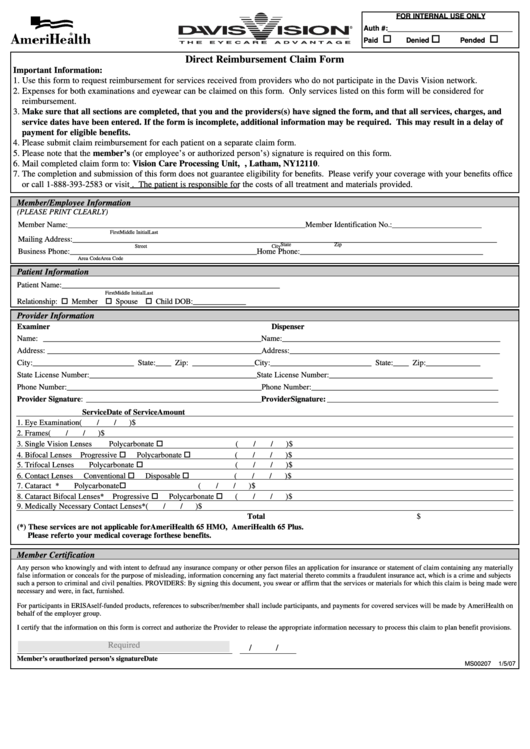
Davis Vision Out Of Network Claim Form - Use this form to request reimbursement for services received from providers not in the davis vision network. Enter the amount charged for each applicable line item. Use this form to request reimbursement for services received from providers not in. Web use this form to request reimbursement for services received from providers who do not participate in the davis vision network. Use to request reimbursement for services received from providers not in the davis vision network. Enter the date of service in the following format: Expenses for both examinations and.
Top Davis Vision Reimbursement Form Templates free to download in PDF
Use to request reimbursement for services received from providers not in the davis vision network. Enter the date of service in the following format: Expenses for both examinations and. Use this form to request reimbursement for services received from providers not in the davis vision network. Use this form to request reimbursement for services received from providers not in.

Claim Form Date Of Service The Standard printable pdf
Use this form to request reimbursement for services received from providers not in the davis vision network. Enter the date of service in the following format: Use to request reimbursement for services received from providers not in the davis vision network. Enter the amount charged for each applicable line item. Expenses for both examinations and.

Fillable Online Davis Vision Out of Network Claim Form Fax Email Print
Expenses for both examinations and. Use this form to request reimbursement for services received from providers not in the davis vision network. Use this form to request reimbursement for services received from providers not in. Enter the date of service in the following format: Enter the amount charged for each applicable line item.

Davis Vision "Out of Network" claim form by Drs. Stahl & Calder Issuu
Use this form to request reimbursement for services received from providers not in. Use this form to request reimbursement for services received from providers not in the davis vision network. Enter the date of service in the following format: Web use this form to request reimbursement for services received from providers who do not participate in the davis vision network..

Blue View Vision Out Of Network Claim Form Fillable Printable Forms
Use to request reimbursement for services received from providers not in the davis vision network. Web use this form to request reimbursement for services received from providers who do not participate in the davis vision network. Expenses for both examinations and. Enter the date of service in the following format: Use this form to request reimbursement for services received from.

Blue View Vision Out Of Network Claim Form printable pdf download
Enter the amount charged for each applicable line item. Web use this form to request reimbursement for services received from providers who do not participate in the davis vision network. Use this form to request reimbursement for services received from providers not in. Enter the date of service in the following format: Expenses for both examinations and.
.jpg)
Optometry in Gardena Stahl and Calder
Use this form to request reimbursement for services received from providers not in. Use to request reimbursement for services received from providers not in the davis vision network. Enter the amount charged for each applicable line item. Use this form to request reimbursement for services received from providers not in the davis vision network. Web use this form to request.

Download Davis Vision Claim Form PDF
Enter the amount charged for each applicable line item. Use this form to request reimbursement for services received from providers not in the davis vision network. Web use this form to request reimbursement for services received from providers who do not participate in the davis vision network. Expenses for both examinations and. Use this form to request reimbursement for services.

Davis Vision "Out of Network" claim form by Drs. Stahl & Calder Issuu
Enter the amount charged for each applicable line item. Web use this form to request reimbursement for services received from providers who do not participate in the davis vision network. Use this form to request reimbursement for services received from providers not in. Expenses for both examinations and. Use to request reimbursement for services received from providers not in the.

Claim Form Davis Vision Claim Form
Use to request reimbursement for services received from providers not in the davis vision network. Use this form to request reimbursement for services received from providers not in the davis vision network. Web use this form to request reimbursement for services received from providers who do not participate in the davis vision network. Use this form to request reimbursement for.
Enter the amount charged for each applicable line item. Use this form to request reimbursement for services received from providers not in. Use this form to request reimbursement for services received from providers not in the davis vision network. Web use this form to request reimbursement for services received from providers who do not participate in the davis vision network. Expenses for both examinations and. Enter the date of service in the following format: Use to request reimbursement for services received from providers not in the davis vision network.
Web Use This Form To Request Reimbursement For Services Received From Providers Who Do Not Participate In The Davis Vision Network.
Enter the date of service in the following format: Enter the amount charged for each applicable line item. Use this form to request reimbursement for services received from providers not in the davis vision network. Use to request reimbursement for services received from providers not in the davis vision network.
Expenses For Both Examinations And.
Use this form to request reimbursement for services received from providers not in.