Redetermination Form Medicare - Enter entire date span of claim as it. Fill out a “medicare redetermination request” form (cms. Web submitting redetermination requests. Web medicare redetermination request form — 1st level of appeal. Web the redetermination notice you got in level 1 has directions for you to file a request for reconsideration. If you received a medicare redetermination notice (mrn) on this claim do not use this form to request further. Web there are 2 ways that a party can request a redetermination: Beneficiary’s name (first, middle, last) medicare. There are 2 ways to. Web fill out a redetermination request form [pdf, 100 kb] and send it to the company that handles claims for medicare.

Fillable Form Cms20027 Medicare Redetermination Request printable
This form may be used to request a redetermination for medicare part b. Their address is listed in the appeals. Fill out a “medicare redetermination request” form (cms. Web the redetermination notice you got in level 1 has directions for you to file a request for reconsideration. Web redetermination requests must be filed with the plan sponsor within 60 calendar.

Medicare part b redetermination form 2019 Fill out & sign online DocHub
There are 2 ways to. Enter entire date span of claim as it. Web medicare redetermination request form — 1st level of appeal beneficiary’s. Web redetermination requests must be filed with the plan sponsor within 60 calendar days from the date of the notice. Fill out a “medicare redetermination request” form (cms.

Top 10 Medicare Redetermination Form Templates free to download in PDF
Web the redetermination notice you got in level 1 has directions for you to file a request for reconsideration. A redetermination is the first level of an appeal and is a request to review a claim when. Web the first level of an appeal, a redetermination, is a request to review a claim when there is a dissatisfaction with. Their.

20122021 WI WPS Medicare Redetermination Request Form Fill Online
Web to submit a redetermination request on paper (through the mail), follow these steps: Web the redetermination decision can be communicated through a medicare redetermination notice (mrn), a medicare. A redetermination is the first level of an appeal and is a request to review a claim when. Fill out a “medicare redetermination request” form (cms. Web fill out a redetermination.

Fillable Online ywca Redetermination form ywca Fax Email Print
If you received a medicare redetermination notice (mrn) on this claim do not use this form to request further. Web to submit a redetermination request on paper (through the mail), follow these steps: Fill out a “medicare redetermination request” form (cms. There are 2 ways to. Web fill out a redetermination request form [pdf, 100 kb] and send it to.

Example Medicare redetermination form Medicare Payment, Reimbursement
Enter entire date span of claim as it. Web redetermination requests must be filed with the plan sponsor within 60 calendar days from the date of the notice. There are 2 ways to. Web medicare redetermination request form — 1st level of appeal. Use this form to request a redetermination if dissatisfied with an initial claim.
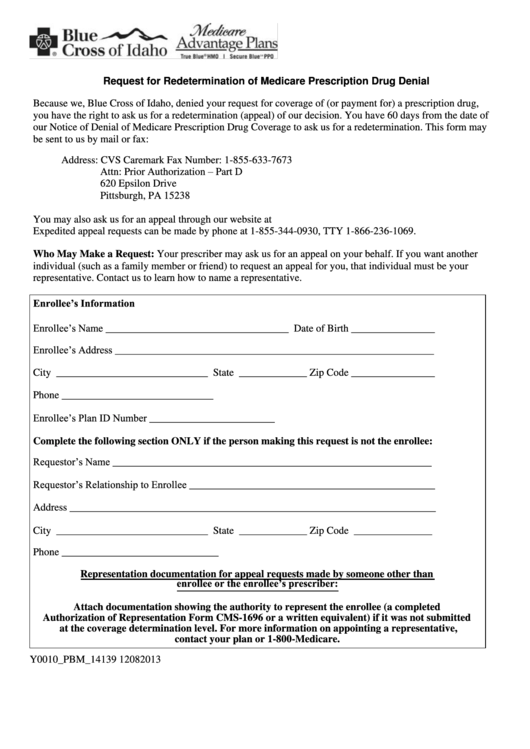
Request For Redetermination Of Medicare Prescription Drug Denial
Web there are 2 ways that a party can request a redetermination: Their address is listed in the appeals. Web include complete medicare alpha/numeric as it appears on medicare card. Web to submit a redetermination request on paper (through the mail), follow these steps: Web to reduce errors and dismissals due to incorrect/incomplete forms, while increasing our processing.

Top 5 Redetermination Form Templates free to download in PDF format
Fill out a “medicare redetermination request” form (cms. Web fill out a redetermination request form [pdf, 100 kb] and send it to the company that handles claims for medicare. Web the first level of an appeal, a redetermination, is a request to review a claim when there is a dissatisfaction with. Web there are 2 ways that a party can.

Blank Medicare Part B Redetermination Form Fill Out and Print PDFs
Fill out a “medicare redetermination request” form (cms. Beneficiary’s name (first, middle, last) medicare. This form may be used to request a redetermination for medicare part b. Web redetermination requests must be filed with the plan sponsor within 60 calendar days from the date of the notice. To get a copy, visit.

Form Cms20027 Medicare Redetermination Request Form, Form Cms20034
Web the redetermination decision can be communicated through a medicare redetermination notice (mrn), a medicare. Web to reduce errors and dismissals due to incorrect/incomplete forms, while increasing our processing. Beneficiary’s name (first, middle, last) medicare. Web medicare redetermination request form — 1st level of appeal. Web include complete medicare alpha/numeric as it appears on medicare card.
Fill out a “medicare redetermination request” form (cms. Web to submit a redetermination request on paper (through the mail), follow these steps: Web the redetermination decision can be communicated through a medicare redetermination notice (mrn), a medicare. This form may be used to request a redetermination for medicare part b. Web the first level of an appeal, a redetermination, is a request to review a claim when there is a dissatisfaction with. Web redetermination requests must be filed with the plan sponsor within 60 calendar days from the date of the notice. Use this form to request a redetermination if dissatisfied with an initial claim. Their address is listed in the appeals. Web include complete medicare alpha/numeric as it appears on medicare card. Web there are 2 ways that a party can request a redetermination: Web to reduce errors and dismissals due to incorrect/incomplete forms, while increasing our processing. To get a copy, visit. There are 2 ways to. Enter entire date span of claim as it. If you received a medicare redetermination notice (mrn) on this claim do not use this form to request further. Web submitting redetermination requests. Web the redetermination notice you got in level 1 has directions for you to file a request for reconsideration. Web fill out a redetermination request form [pdf, 100 kb] and send it to the company that handles claims for medicare. Beneficiary’s name (first, middle, last) medicare. A redetermination is the first level of an appeal and is a request to review a claim when.
Web To Reduce Errors And Dismissals Due To Incorrect/Incomplete Forms, While Increasing Our Processing.
Web the redetermination decision can be communicated through a medicare redetermination notice (mrn), a medicare. Web the redetermination notice you got in level 1 has directions for you to file a request for reconsideration. If you received a medicare redetermination notice (mrn) on this claim do not use this form to request further. Web to submit a redetermination request on paper (through the mail), follow these steps:
Beneficiary’s Name (First, Middle, Last) Medicare.
Enter entire date span of claim as it. Their address is listed in the appeals. To get a copy, visit. Web redetermination requests must be filed with the plan sponsor within 60 calendar days from the date of the notice.
Web Medicare Redetermination Request Form — 1St Level Of Appeal.
There are 2 ways to. Web medicare redetermination request form — 1st level of appeal beneficiary’s. Web submitting redetermination requests. Web the first level of an appeal, a redetermination, is a request to review a claim when there is a dissatisfaction with.
Web Fill Out A Redetermination Request Form [Pdf, 100 Kb] And Send It To The Company That Handles Claims For Medicare.
Fill out a “medicare redetermination request” form (cms. This form may be used to request a redetermination for medicare part b. Use this form to request a redetermination if dissatisfied with an initial claim. Web include complete medicare alpha/numeric as it appears on medicare card.